A diagnosis, and the beginnings of treatment...
In December 2005 I saw a pain management specialist who confirmed the diagnosis of Complex Regional Pain Syndrome, or CRPS. I didn’t like him and wasn’t comfortable with him. It seems that all the doctors in this field have their eccentricities; this one particularly so. At that stage, all he did was send me to see a physiotherapist who specialised in the condition. Almost the first thing the physio told me was that I should drop out of uni because a career as a vet wasn't suitable for somebody with CRPS. He showed me some techniques – Mirror Imagery (MI) and Graded Motor Imagery (GMI) - that can be valuable in treating CRPS, but these didn't help me. I gave up seeing him fairly quickly. It was too far to travel, he wasn’t helping my leg and he was making me feel worse in myself.
Within a few months my leg began to get worse. Around April 2006, my pain became so severe that I found myself on crutches as it was becoming almost impossible to weight-bear normally. My whole leg had become swollen and horribly discoloured and the pain was like nothing I had ever known. I had a final follow-up with the surgeon and he contacted a different specialist then and there, who agreed that we needed to do something straightaway. He scheduled my first lumbar sympathetic nerve block for the following week as I sat in the surgeon’s consulting room.
One of the main theories of CRPS is that it involves dysfunction of the sympathetic nervous system, which is thought to account for the main visible signs of the condition: the oedema, the colour change, temperature change, etc. There are numerous theories out there related to Sympathetically Maintained Pain (SMP) and Sympathetically Independent Pain (SIP), the thought process being that with time, other processes take over and the role of the sympathetic nervous system becomes less important. This may explain why sympathetic nerve blocks can bring great relief, even remission, for one CRPS patient, yet have no effect at all upon another.
Blocks are done in different ways, depending on the individual doctor. I remember nothing of mine as it was done under a light general anaesthetic. It did have a very short-lived effect but I didn’t really have much pain relief, and what little I had had worn off almost by the time I left the hospital – just two or three hours later. I had some improvement in the colour and temperature of my leg, but that too had worn off within a few hours. Based on this result, my specialist decided to do a prolonged block, which meant a few days in hospital with a catheter in my back providing continuous anaesthesia to the sympathetic nerve. Again I had initial relief, but the effects began to wear off within a couple of days, even while the block remained in place.
My leg continued to deteriorate quickly - previously, although the oedema and colour change had involved my knee and lower leg, the pain had been mainly confined to my knee. One night, I was lying on the couch and was sure that I could feel a pin sticking into my big toe. When I went searching for it, I realised that it was a loose thread on the throw-rug brushing against my toe. Over the next two week, my toes and foot developed the same burning pain and hypersensitivity as in my knee and over about a month the pain coalesced so that I had a ‘stocking’ of pain from mid-thigh right down to my toes.
|

|
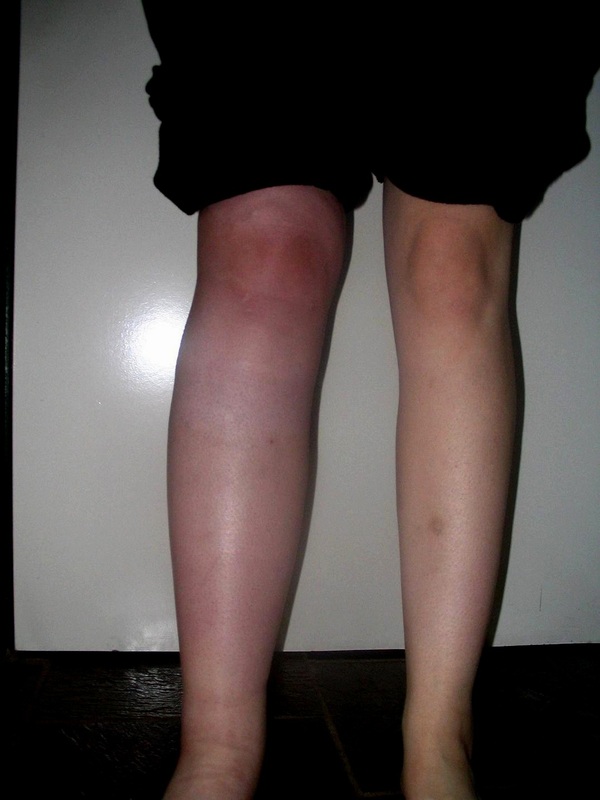
Deterioration in my right leg from May 2006 to early July 2006 despite treatment with sympathetic nerve blocks.
My specialist started me on amitriptyline, which is a type of antidepressant known to have efficacy against neuropathic pain such as that caused by CRPS. It did nothing for my pain, but left me feeling anxious, sick and hung-over to the point that I really didn’t want to take it.
It was at this stage that he suggested I think about the possibility of trialling a spinal cord stimulator. A spinal cord stimulator (SCS) is an implanted device not dissimilar to a cardiac pacemaker, only it provides pain relief. Electrodes are implanted in the epidural space – over the spinal cord – and connected via a lead to a battery and implantable pulse generator (IPG) implanted over the abdomen. The IPG creates electrical impulses that interfere with nerve signalling, which creates a tingling sensation in the painful areas. It doesn’t get rid of the pain, but when it’s working, it helps to relieve it.
I decided to undergo a trial stimulation period. These involved having the electrode and lead implanted in my spine and connected to an external pulse generator. The surgery is rather unpleasant; because the electrode must be placed to give an optimal stimulation for each individual patient, you have to be awake when they place it so that they can stimulate and you can give feedback on where you are getting coverage. Once the electrode had been placed, the lead was channelled through my side and attached to the external unit. My technician began programming and after a couple of days in hospital I went home to try to ascertain whether the SCS was a reasonable option for me.
It didn’t eliminate my pain, and in fact didn’t really touch some elements of it at all. What it did do was reduce the allodynia, or extreme sensitivity to touch. Within a couple of months I progressed from a leg so sensitive that I couldn’t even wear long pants, never mind a sock or shoe, to being able to weight bear with crutches.
It was at this stage that he suggested I think about the possibility of trialling a spinal cord stimulator. A spinal cord stimulator (SCS) is an implanted device not dissimilar to a cardiac pacemaker, only it provides pain relief. Electrodes are implanted in the epidural space – over the spinal cord – and connected via a lead to a battery and implantable pulse generator (IPG) implanted over the abdomen. The IPG creates electrical impulses that interfere with nerve signalling, which creates a tingling sensation in the painful areas. It doesn’t get rid of the pain, but when it’s working, it helps to relieve it.
I decided to undergo a trial stimulation period. These involved having the electrode and lead implanted in my spine and connected to an external pulse generator. The surgery is rather unpleasant; because the electrode must be placed to give an optimal stimulation for each individual patient, you have to be awake when they place it so that they can stimulate and you can give feedback on where you are getting coverage. Once the electrode had been placed, the lead was channelled through my side and attached to the external unit. My technician began programming and after a couple of days in hospital I went home to try to ascertain whether the SCS was a reasonable option for me.
It didn’t eliminate my pain, and in fact didn’t really touch some elements of it at all. What it did do was reduce the allodynia, or extreme sensitivity to touch. Within a couple of months I progressed from a leg so sensitive that I couldn’t even wear long pants, never mind a sock or shoe, to being able to weight bear with crutches.
